








Tom Neltner, J.D. is the Chemicals Policy Director.
This month, the Food and Drug Administration (FDA) released its “Closer to Zero” action plan to reduce exposure to heavy metals in foods for babies and young children. The plan, released in response to a recent House of Representatives Committee on Oversight and Reform report and the introduction of the Baby Food Safety Act in both the House and the Senate, is a step forward since it commits the agency to specific actions and general deadlines for the first time. However, there is room for improvement, specifically the agency should:
- Explicitly consider the cumulative effect of heavy metals on neurodevelopment when setting limits.
- Move up deadlines for draft action levels for arsenic and cadmium;
- Be consistent in messaging that there is no safe level of lead in children’s blood;
- Define what “as low as possible” and “children’s food” means as soon as possible;
- Be transparent by posting testing data quickly; and
- Add milestones for compliance verification with action levels and preventive controls.
FDA’s plan must address the cumulative effect of arsenic, cadmium, lead, and mercury in food
When FDA announced a new Toxic Elements Working Group following a critical report by the Government Accountability Office three years ago, Dr. Susan Mayne, FDA’s director for the Center for Food Safety and Applied Nutrition said the group was “charged with identifying, targeting, and prioritizing our efforts to achieve the public health goal of reducing exposure to toxic elements to the greatest extent possible.” The point person on the effort, Dr. Conrad Choiniere, described it as “taking a more strategic, global approach — looking at all the metals across all foods rather than one contaminant, one food at a time.” He explained that the agency was focused “first on metals like lead, arsenic, cadmium, and mercury in foods, cosmetics, and dietary supplements. These naturally occurring contaminants are present in many of the foods we eat, but can be especially harmful to children because of concerns about effects on their neurological development.”
At the time, we applauded FDA’s focus on the cumulative effect of these four heavy metals on children’s brain development because they are not exposed to them in isolation. Many individual foods contain more than one, and they are all too common in foods across the diet. FDA’s own Total Diet Study (TDS) data as well as Consumer Reports’ 2018 report and Healthy Babies Bright Future’s 2019 report show that many foods have multiple heavy metals. And, as Dr. Choiniere clearly explained, “even though the levels of a metal in any particular food is low, our overall exposure adds up because many of the foods we eat contain them in small amounts.”
Unfortunately, in the Closer to Zero plan issued three years after the working group was created, FDA does not address the issue of the cumulative effects of heavy metals in the diet. Instead, the agency’s milestones address the risk one contaminant at a time, starting with draft action levels for lead by April 2022, arsenic by April 2024, and cadmium and mercury at an undefined later date. The sequential approach makes it difficult to consider the combined effects. Ideally, they would be issued together.
In addition, the plan’s research activities and associated milestones do not address the issue. The omission is surprising because the agency’s own scientists have conducted innovative studies suggesting that when mercury is present, the adverse effects of arsenic, cadmium, and lead are worse; they also showed that arsenic and cadmium have additive effects. While more research is needed, the data reinforce the need for FDA to expressly account for the cumulative effect when setting limits.
We recommend that the agency address the cumulative effect of heavy metals on neurodevelopment by:
- Explicitly considering the issue when setting Interim Reference Levels (IRLs) and deriving action levels;
- Presuming an additive effect unless there is evidence to the contrary; and
- Adding to its research milestones an annual update on the state of the evidence on cumulative effects and its progress in filling information gaps.
FDA must move up deadlines for arsenic and cadmium action levels
In the plan, FDA’s deadline to propose draft action levels for arsenic is April 2024. There is no deadline for cadmium and mercury. Those timelines need to be accelerated.
For arsenic, the agency finalized an action level for inorganic arsenic in infant rice cereal in 2020 and plans to do the same for apple juice this year. However, the draft action levels were proposed in 2016 and 2013 respectively. It took so long that the risk assessment on which the proposals were based is already outdated. In the intervening years, the evidence of arsenic exposure and neurological harm which was deemed insufficient to quantify the risk five years ago has become even more compelling.
In addition, FDA reports that manufacturers have made significant progress in reducing arsenic in infant rice cereal since 2011. From FDA’s TDS, we have seen similar results for arsenic in juices. Given the progress, the agency should evaluate the possibility of tightening the levels further and on a faster timeline so they are public by April 2022.
For cadmium, while FDA’s scientists have made progress on its research since the launch of the Toxic Elements Working Group in 2017, it has yet to translate its results into action. In 2019, it assessed children’s exposures to cadmium (and lead) based on the agency’s TDS but did not propose an Interim Reference Level (IRL) – a measure of the amount of a substance in the diet that could result in a specific health impact. This is especially concerning as our review of the study showed that the average young child exceeds relevant exposure limits set by other agencies and exposure to cadmium was three to four times greater than lead. A year later, agency scientists summarized the evidence regarding best practices to reduce cadmium and identified specific mitigation strategies demonstrated to be effective. Clearly, the agency has sufficient information to move forward with draft action levels and should proposed those no later than April 2023.
FDA needs to be consistent in messaging that there is no safe level of lead in children’s blood
In announcing the plan, FDA’s acting commissioner Dr. Janet Woodcock and Center for Food Safety and Applied Nutrition’s (CFSAN) director Dr. Susan Mayne twice stated that “FDA’s testing shows that children are not at an immediate health risk from exposure to toxic elements at the levels found in foods.” The language gives parents a false assurance that there no real risk of harm to a child’s brain from exposure to lead in food. While the harm from a short-term, low-level exposure to lead cannot be measured in a single child, when many children are evaluated, the risk is unmistakably clear.
FDA’s webpage on lead in food clearly states “there is no identified safe blood lead level” and that “Lead is especially harmful to vulnerable populations, including infants, young children, pregnant women and their fetuses.” This accords with the American Academy of Pediatrics (AAP) statement that “there is no safe level of lead exposure in children.” Similarly, the Centers for Disease Control and Prevention (CDC) says “no safe blood lead level in children has been identified” as do the Environmental Protection Agency and the Center for Medicaid and Medicare Services.
FDA’s “no immediate health risk” statement may be designed to reassure the public but only serves to undermine the agency’s credibility on the issue. We saw a similar glossing over in a February 2020 study by its own scientists. In the study, the authors reviewed the evidence the agency used to support its 2018 Interim Reference Level (IRL) of 3 µg/day of lead for children. The abstract states that:
“The literature review showed that no adverse effects of lead consistently occurred at the BLL [blood lead level] associated with the IRLs (0.5 μg/dL). The IRLs of 3 μg/day for children and 12.5 μg/day for [Women of Child-Bearing Age] should serve as useful benchmarks in evaluating the potential for adverse effects of dietary lead.”
Unfortunately, the authors’ broad statement in the abstract fails to mention that they specifically excluded harm to children’s brain development from their analysis of adverse effects. They said, “neurodevelopment was excluded as an endpoint in the literature review because no safe level with respect to this endpoint has been identified to date.”
We understand that the agency needs a numerical value as a starting point to initiate measures to bring that value to levels closer to zero. However, FDA’s messaging should be consistent that the IRLs and action levels are not “safe” levels.
FDA should define scope of food potentially affected and what “as low as possible” means as soon as possible
In announcing the plan, Commissioner Woodcock and CFSAN Director Mayne described the agency’s “approach to reducing exposure to toxic elements in foods commonly eaten by babies and young children to the lowest possible levels.” We support this objective but recognize that two key terms need to be defined more clearly for the effort to stay on track and succeed.
First, “foods commonly eaten by babies and young children” can be interpreted in many different ways. It clearly goes beyond only those foods specifically marketed for infants and toddlers. In addition, for lead, young children are generally defined as those up to six years of age. We support a broad definition and encourage FDA to define the scope quickly to help ensure the agency gets the information it needs to set useful limits.
Second, “as low as possible” is vague. We have seen how Codex Alimentarius has set a low bar for “possible” by establishing international standards for lead in apple juice of 30 parts per billion (ppb) and grape juice of 40 ppb based on what approximately 90% of the products on global marketplace can achieve. Codex’s market assessment did not consider whether the companies were applying preventive controls or best practices to reduce the contamination levels – something FDA has pledged to do in its March announcement.
We think that adopting Codex’s flawed approach would be insufficient in the United States. FDA needs to drive the market further and consider only levels in ingredients made using best practices that reduce children’s exposure when setting its standards. These best practices must include changes to how we grow, harvest, and process foods like rice, sweet potatoes, carrots, quinoa, and fruits.
An early test of FDA’s commitment will come when it releases the draft action levels for lead in juices as described in the plan. Setting levels above 5 ppb will be difficult to defend based on the TDS data from 2014-17.
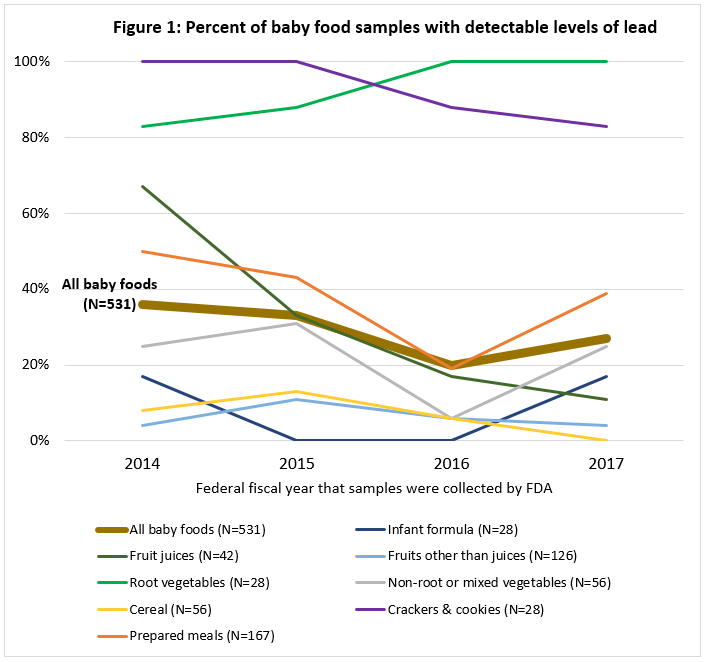{kind=link}
While the agency will no doubt address the issue when it meets the April 2022 milestone for action levels for lead, we encourage FDA to define these critical terms earlier in the process to help guide efforts to reduce heavy metals in food.
FDA should add milestone for compliance verification with action levels and preventive controls
The plan identifies “increasing targeted compliance and enforcement activities” as one of five key strategies to reduce heavy metals in food. FDA took a modest step in that direction when it sent a letter to industry last month reminding baby food manufacturing of their existing responsibilities in its Prevention Controls rule to address chemical hazards, including, heavy metals, in their Food Safety Plans.
Moreover, February’s House Committee on Oversight and Reform report made clear greater compliance assurance is needed by FDA’s Office Of Regulatory Affairs in coordination with CFSAN. Therefore, we recommend that FDA add specific annual compliance verification milestones to the plan.
FDA should be transparent by posting testing data quickly
In the plan, FDA says it “is committed to a science-driven, transparent, and inclusive process that will include active stakeholder engagement and public sharing of data and information.” We applaud that commitment.
We encourage the agency to release its testing data as it becomes available after assuring its quality instead of releasing as part of a formal decision. This includes prioritizing the release of its TDS testing data from 2018 and 2019 for the four heavy metals and provide frequent updates as the agency conducts the various studies described in the plan. The agency took this approach for per- and polyfluorinated alkyl substances to a positive effect. This approach will allow it to fulfill its commitment to active stakeholder engagement more effectively. As importantly, it will allow companies to act on the most recent data as they update their preventive controls through the Food Safety Plans.
Summary
The Closer to Zero plan is a step forward because it commits the agency to specific actions and general deadlines for the first time. We identify five areas for improvement with specific suggestions for each. However, given the agency’s track record taking years to even propose draft action levels – levels that are not sufficiently protective for children –and the challenges moving forward, we anticipate continued Congressional oversight and action and targeted appropriations will be needed to ensure that levels of heavy metals in children’s food really do get closer to zero.